If your AI system can affect patient care, billing, or PHI, I’d treat ISO 42001 as a governance system - not just a policy document.
Here’s the short version: I’d use ISO 42001 to put AI under clear ownership, rank systems by risk, require impact reviews before launch, monitor models after release, and tighten vendor checks. In healthcare, that matters because one weak model can affect diagnosis, triage, privacy, or claims at scale.
What this means for you:
- Start with high-risk AI first: CDS, imaging, triage, ambient scribing, and patient chat tools
- Set clear ownership: board, clinical, security, privacy, legal, and compliance roles
- Require two reviews before launch: business risk review and person-impact review
- Control the full lifecycle: design, testing, release, monitoring, retraining, and retirement
- Watch for common failure points: bias, drift, weak explainability, PHI misuse, model abuse, and vendor changes
- Keep proof: inventory, model cards, validation records, incident logs, and change records
- Check third-party vendor risk hard: data lineage, update notices, rollback plans, SLAs, and audit evidence
A few points stand out. ISO 42001 is certifiable, unlike NIST AI RMF. It uses a plan-do-check-act model. And it fits healthcare because AI risk is not just an IT issue - it can become a patient safety issue fast.
Quick comparison
| Area | ISO 42001 | NIST AI RMF |
|---|---|---|
| Type | Requirements-based management system | Guidance framework |
| Certification | Yes | No |
| Main use | Governance, audit proof, role-setting | Risk mapping and analysis |
| Best fit in healthcare | Enterprise AI oversight | Technical risk review |
I’d read the rest of the article as a playbook for building an AI management system that connects clinical review, privacy, security, vendor control, and audit evidence in one process.
ISO 42001 vs NIST AI RMF: Healthcare AI Governance Comparison
Understanding ISO 42001 in Healthcare AI Contexts

What ISO/IEC 42001 Is and Why It Was Created
ISO/IEC 42001 applies a management-system model to AI governance through Plan-Do-Check-Act (PDCA) [8][4].
Put simply, it treats AI governance like a system that has to be planned, run, reviewed, and improved over time. That matters in healthcare, where AI can affect patient safety, privacy, and clinical decisions in very direct ways.
Unlike internal policies or voluntary guidance, ISO 42001 is certifiable; third-party auditors can validate an AIMS and provide independent proof of governance [3][5]. For healthcare teams, that means they can show auditable oversight of AI systems across the full lifecycle, not just say they have rules on paper.
Core ISO 42001 Principles That Apply to Healthcare
ISO 42001 is built around several principles that line up closely with the biggest AI concerns in healthcare.
Accountability and leadership come first. The standard requires board-level oversight and clearly defined roles for AI safety and ethics, including escalation paths when clinical risks emerge [3][9]. In plain English: someone has to own the risk, and there has to be a clear path for action when something starts to go wrong.
AI Impact Assessments (AIIAs) are one of the standard's standout elements. For high-risk healthcare applications, organizations must assess impacts across eight dimensions: accountability, transparency, fairness, privacy, reliability, safety, explainability, and environmental impact [6][9]. These impact assessments are detailed and substantial, evaluating effects on individuals, groups, and society as a whole - a significant departure from similar ISO standards.
That’s a big deal in healthcare. A model doesn’t just affect a workflow. It can shape triage, treatment choices, access to care, and how patient data is handled.
Lifecycle management is another core requirement. Controls must span all seven stages of an AI system's life: Inception, Design/Development, Verification/Validation, Deployment, Operation/Monitoring, Re-evaluation, and Retirement [6]. This is especially important in healthcare, where a model's performance can degrade over time through model drift.
If you’ve ever seen a tool work well at launch and then slowly slip as patient populations, workflows, or data inputs change, that’s the risk this is trying to address.
It also aligns with ISO 13485, ISO 27001, and ISO 27701 for quality, security, and privacy [3].
How ISO 42001 Differs from Guidance-Based AI Frameworks
In healthcare, the key issue isn’t whether AI helps. It’s how the risks are governed. The NIST AI Risk Management Framework (AI RMF) is the most common comparison point.
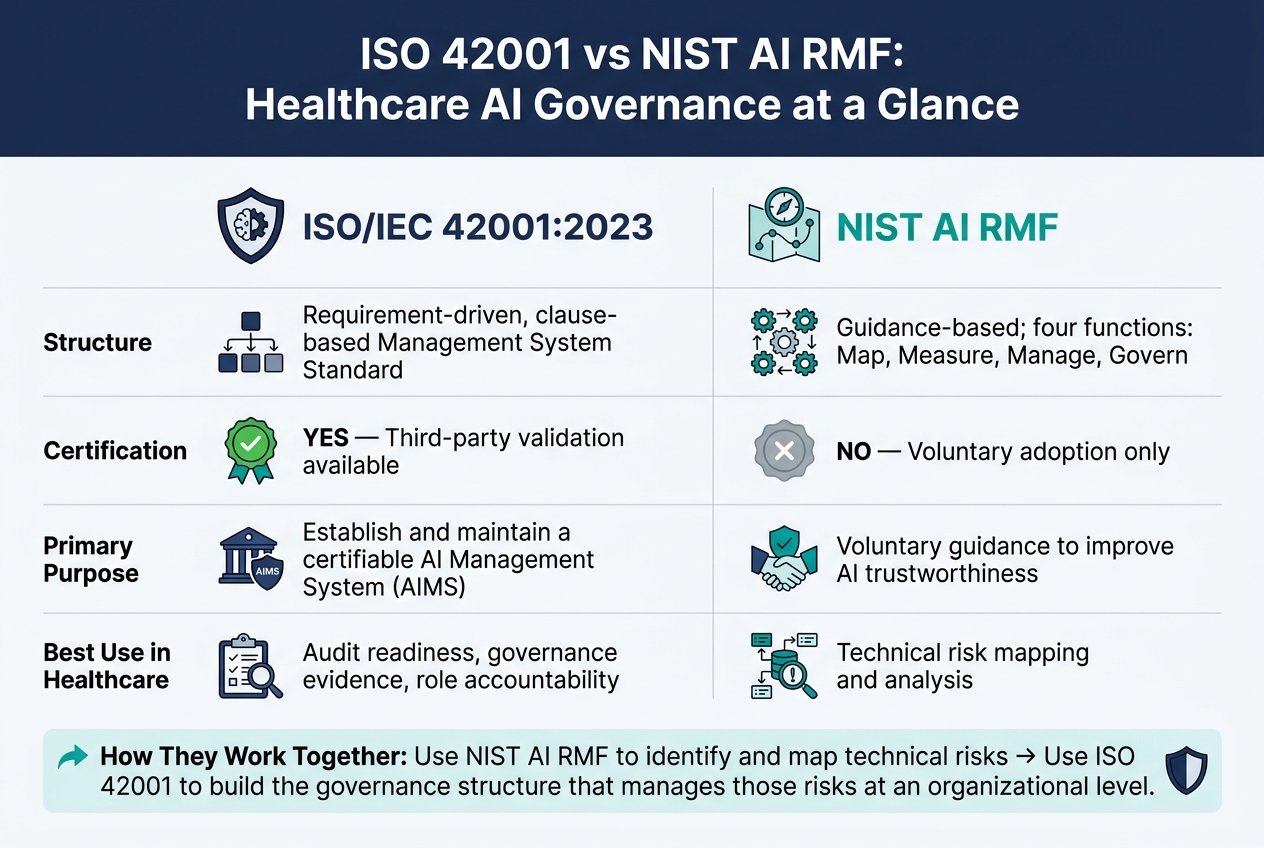
| Feature | ISO/IEC 42001:2023 | NIST AI RMF |
|---|---|---|
| Structure | Requirement-driven, clause-based Management System Standard | Guidance-based; four functions: Map, Measure, Manage, Govern |
| Purpose | Establish and maintain a certifiable AIMS | Voluntary guidance to improve AI trustworthiness |
| Certification | Yes - third-party validation available | No - voluntary adoption only |
| Healthcare Use | Audit readiness and governance evidence | Technical risk mapping |
In practice, these frameworks are not mutually exclusive. Many healthcare organizations use the NIST AI RMF to identify and map specific technical risks, then use ISO 42001 to build the governance structure that manages those risks at an organizational level.
That split makes sense. NIST helps teams see the risk. ISO 42001 helps them prove they have a system for handling it.
For healthcare organizations, ISO 42001 provides auditable evidence of AI governance for compliance, procurement, and review. This process is streamlined when teams use automated tools to answer security questionnaires and map evidence to these standards. That governance layer becomes practical when mapped to clinical, operational, and vendor risk.
sbb-itb-535baee
What ISO 42001 Means for Healthcare Compliance
Mapping ISO 42001 Requirements to Healthcare AI Risks
With the framework in place, the next move is to map ISO 42001 controls to the risks tied to each healthcare AI use case.
Healthcare AI Use Cases and Their Risk Profiles
Healthcare AI covers a wide range of use cases, and those use cases do not carry the same level or type of risk. ISO 42001 only works if the controls fit the system being used.
Clinical decision support (CDS) tools help with diagnosis, medication dosing, and treatment planning. The main risks are unsafe outputs and limited explainability. If a clinician can’t make sense of a model’s output, it gets much harder to check it or push back when it’s wrong. ISO 42001 addresses this through human oversight requirements (Annex A.6.1) and transparency controls (Annex A.8.3) [3][7].
Imaging and pathology AI is especially exposed to drift. Radiology and pathology models can shift as patient populations, medical device equipment, or clinical protocols change. Continuous performance monitoring under Annex A.10.3 is meant to catch that kind of decline before it reaches patients [3][10].
Ambient documentation tools that record and transcribe clinical conversations bring PHI exposure risk. ISO 42001’s data governance controls (Annex A.7.2) and privacy-by-design principles line up closely with HIPAA safeguards in this area [1][10].
Patient-facing chatbots bring ethical and safety risks that teams sometimes miss. Bad information or biased responses can lead to direct harm. ISO 42001 maps these issues to transparency requirements (Annex A.8.2) and safety filters or guardrails (Annex A.8.4) [6][7].
Revenue cycle automation creates workflow and auditability risk, especially when automated decisions affect billing or scheduling [7][10].
Risk Categories ISO 42001 Helps Address
ISO 42001 splits AI risk into two separate obligations: Clause 6.1.2 for organizational risk and Clause 6.1.4 for societal and individual impact [7]. That split matters in healthcare because one AI system can create an operational problem for the organization and, at the same time, a direct patient safety issue.
ISO 42001 addresses bias, explainability, drift, misuse, privacy, and broader impact across both people and operations.
In healthcare, the six main risk categories it helps address are clinical safety and efficacy, ethical and social harms including bias and health equity, data privacy and HIPAA compliance, cybersecurity and model integrity, model reliability, and operational disruption. Each of these can lead to patient harm, regulatory trouble, or both.
For cybersecurity, ISO 42001 connects with ISO/IEC 27001 and supports threat-modeling methods like STRIDE to spot vulnerabilities such as prompt injection or unauthorized model access (Annex A.8) [3][6]. For bias and health equity, the standard supports fairness testing, balanced training data, and impact assessments used to review discrimination and exclusion risks (Annex A.6.2.2, A.7.4) [7].
How ISO 42001 Requirement Areas Align to Healthcare Risk Domains
These risk categories line up directly with the standard’s main requirement areas. The table below turns ISO 42001 clauses into governance actions healthcare teams can use.
| ISO 42001 Requirement Area | Healthcare Governance Application | Practical Example |
|---|---|---|
| Context (Clause 4) | AI Governance Committees | Defining which clinical and operational systems fall in scope [1] |
| Leadership (Clause 5) | Board-level Oversight | Assigning clear accountability for AI risk [3] |
| Planning (Clause 6) | Risk Appetite & AIIAs | Requiring impact assessments before deployment [6] |
| Support (Clause 7) | Clinician Training & Resources | Educating staff on the limits and explainability of CDS tools [7] |
| Operations (Clause 8) | Model Validation & Lifecycle | Implementing change control for model updates in revenue cycle software [3] |
| Performance (Clause 9) | Monitoring & Audit Evidence | Monitoring live performance metrics for drift and error rates [3][6] |
| Improvement (Clause 10) | Incident Response & CAPA | Analyzing near-miss clinical events caused by AI to update safety filters [7] |
These mappings only become useful when teams build them into day-to-day governance, assessment, and monitoring routines.
Classify systems by risk so high-risk clinical AI gets deeper controls than administrative automation.
Building an AI Management System for Healthcare
Turn the risk map above into an operating model.
Define Governance, Scope, and AI Risk Appetite
The first step is simple: decide what belongs inside your AI Management System, or AIMS, and who is on the hook for it. Start by sorting AI systems by impact. Put high-impact systems at the front of the line. That includes systems that affect patient safety, clinical eligibility, financial outcomes, or handle Protected Health Information (PHI).
Once you’ve set scope, create an executive AI governance council with people from clinical, IT, security, privacy, legal, and regulatory affairs. That gives you cross-functional oversight from day one. If PHI is involved, connect the AIMS to HIPAA safeguards and to your current security and privacy management systems, such as ISO 27001 and ISO 27701 [1]. And if an AI tool is used for diagnosis, triage, or treatment planning, the risk appetite statement should clearly say that human oversight is required.
A 60-day launch plan works well here:
- Weeks 1–2: scope and inventory
- Weeks 3–4: assessment methods
- Weeks 5–6: controls
- Weeks 7–8: tabletop review and management sign-off
Build a Healthcare-Specific AI Risk Assessment and Treatment Process
Every AI system should be cataloged, including any Software as a Medical Device (SaMD). For each one, record its business purpose, intended use, data types processed, model owner, hosting location, monitoring approach, and the date of its last risk assessment. Just as important, set a rule that no new AI tool goes to production until it has been registered in the AIMS inventory.
Before deployment, complete both the organizational risk assessment and the AIIA. Clause 6.1.2 covers operational risk, and Clause 6.1.4 covers patient and societal impact [7].
The table below links common healthcare AI risk scenarios to ISO 42001 control areas and practical mitigations [7]:
| Risk Category | Healthcare Example Scenario | ISO 42001 Control Area | Mitigation |
|---|---|---|---|
| Bias & Fairness | Diagnostic tool underperforms on specific demographic cohorts | A.6.2.2, A.7.4 | Balanced training data; fairness testing; clinician review |
| Explainability | Triage model cannot justify a "high-risk" score to a physician | A.8.2, A.8.3 | Interpretable models; model cards; user documentation |
| Safety | Autonomous robotic system behaves unexpectedly during surgery | A.6.2.4, A.9.4 | Staged rollout; shutdown controls; continuous human oversight |
| Privacy | Training data contains PHI used without proper de-identification | A.7.2, A.8.2 | Data minimization; anonymization; HIPAA risk analysis and privacy review |
| Operational Drift | Sepsis alert model loses accuracy after 6 months | A.6.2.6, A.6.2.8 | Drift detection; retraining triggers; performance dashboards |
| Supply Chain | A third-party LLM provider updates its API, breaking a clinical bot | A.10.2, A.10.4 | Supplier due diligence; fallback providers; contractual SLAs |
For technical risk discovery, use STRIDE at each lifecycle stage. That helps teams look for spoofing, tampering, repudiation, information disclosure, denial of service, and elevation of privilege [6]. For high-risk clinical AI deployments, clinician review should be part of protocol validation and explainability evidence review [1].
Apply Lifecycle, Documentation, and Monitoring Controls
Once inventory and assessment are in place, bake controls into each lifecycle stage. The table below shows the key controls and the evidence you should keep:
| Lifecycle Stage | Key ISO 42001 Controls | Required Evidence |
|---|---|---|
| Inception | Governance roles (A.6.1), scope definition | AI project inventory, risk appetite statement |
| Design & Development | Data governance (A.7.4), tampering protection | Data lineage records, STRIDE threat models |
| Verification | Traceability (A.8.5), clinical validation | Validation protocols, bias assessment reports |
| Deployment | Access control (A.10.2), release management | Deployment logs, user-facing documentation |
| Operation | Drift monitoring (A.6.2.6), security (A.8.3) | Performance dashboards, incident logs |
| Re-evaluation | Change control (A.10.2), model retraining | Change summary artifacts, management reviews |
| Retirement | Decommissioning (A.9.4) | Decommissioning reports, final audit logs |
For every high-impact system, keep a model card as governance evidence for monitoring, audit, and review. It should record the system’s purpose, performance metrics, known limits, training data lineage, and clinical validation results.
For change management, require a change summary artifact before any update moves to production. That artifact should say what changed, how the risk impact was assessed, and what testing evidence supports the update.
On monitoring, set clear statistical thresholds for model drift that automatically trigger re-evaluation or retraining [7]. Use a centralized RiskOps workflow so findings, owners, and due dates move cleanly across governance teams. That way, audit readiness becomes part of day-to-day work instead of a last-minute scramble before review.
Next, extend the same controls to vendors, compliance, and ongoing improvement.
Running ISO 42001 Across Vendors, Compliance, and Ongoing Improvement
Assess Readiness and Prioritize High-Risk AI Systems
Once lifecycle controls are in place, the next step is showing that the program holds up in day-to-day use: readiness, audits, and vendor oversight. A gap assessment compares your current policies, controls, and documentation against ISO 42001 requirements. From there, map your current HIPAA and FDA controls to ISO 42001, then focus first on the AI systems with the highest patient safety impact and the greatest PHI exposure [2][3].
Before you go after third-party certification, run at least one full internal audit and one management review. Your CAPA log should include real findings, named owners, and closure dates - not placeholders [11].
Internal readiness is only half the picture. Third-party AI can bring risk back in faster than internal controls can handle it.
Manage Third-Party AI Risk and Supply Chain Oversight
In healthcare, a lot of AI risk sits outside your organization. Foundation model providers, clinical AI vendors, and cloud infrastructure partners all add risk that your AIMS needs to address under Annex A.10.
Due diligence needs to go past the usual security questionnaire. Review third-party models for data lineage, training-data representativeness, and shutdown capability [3][7]. ISO 42001 certification is starting to look like a baseline expectation for AI vendors working in regulated healthcare settings.
Contracts help, but they don't solve everything. You can transfer financial liability on paper, but you can't fully hand off regulatory accountability for patient data to a supplier [7]. So your team needs ongoing monitoring, not just a signed agreement.
Ask vendors to notify you about model updates that could change clinical behavior. Set clear thresholds for retraining, rollback, or decommissioning when model drift or performance degradation shows up [7][12]. If you're dealing with a large vendor portfolio, platforms like Censinet RiskOps™ can centralize third-party and enterprise risk assessments, along with evidence review.
Conclusion: ISO 42001 as a Working Model for Healthcare AI Governance
That model only works if procurement, monitoring, and remediation stay tied together.
ISO 42001 gives healthcare organizations something many AI guidance frameworks do not: a certifiable, auditable management system with defined controls, documented evidence requirements, and clear accountability. It maps directly to U.S. healthcare obligations - HIPAA Privacy and Security Rules, FDA expectations for SaMD, and the NIST AI RMF - without forcing teams to build a separate governance program from scratch [2][7][13]. It gives clinical teams, procurement reviewers, and executive leadership a shared way to talk about AI risk, based on evidence rather than assurances. ISO/IEC 42001 is the governance analog to ISO 27001: a sign of maturity, not a guarantee of safety [14].
The goal is a working model that clinicians, compliance teams, and vendors can use and improve with each audit cycle.
FAQs
Who should own ISO 42001 in a healthcare organization?
ISO 42001 should have executive ownership so leadership is on the hook for decisions and oversight. The standard asks for more than one named person handling the work.
In healthcare, AI governance comes with complex risks. That’s why organizations should rely on a cross-functional team, with people from informatics, legal, data analytics, privacy, patient experience, equity, quality, and safety at the table.
Which healthcare AI tools should be prioritized first?
Healthcare organizations should put high-risk AI systems at the top of the list, especially the ones that can change patient care or safety in a direct way.
Start with a full inventory of every AI system in use now, plus any that are planned. Then sort those systems by risk level. From there, give first attention to critical tools like clinical diagnostic systems, medical imaging AI, patient monitoring systems, and clinical decision support systems.
How does ISO 42001 support HIPAA and FDA compliance?
ISO 42001 supports HIPAA and FDA compliance by giving organizations a structured, auditable way to govern AI risk.
For HIPAA, it helps teams document how AI systems use protected health information, track changes over time, and monitor those systems on a regular basis. That paper trail matters. If an AI tool touches PHI, you need to know what it’s doing, who changed it, and whether it’s still operating as expected.
It also lines up well with FDA quality and safety goals. In practice, that means using AI impact assessments and lifecycle controls to keep models stable, reduce bias, and watch for drift or other performance issues over time.
